
Historically, miniature radiography for mass Tuberculosis (TB) screening activities was widely utilised in high-income countries throughout the 20th century. In lower-and middle income countries (LMIC), like Kenya, chest X-ray (CXR) has been used primarily as a complementary tool to support clinical diagnosis of TB. With findings of CXR being a good screening tool during the TB prevalence surveys, the conversations have shifted to having CXR screening earlier in the screening and triaging cascade.
World Health Organisation (WHO) in 2016 developed a guidance of CXR use for TB screening and triaging. Subsequently this year (2021), further guidelines on systematic TB screening were released recommending TB screening using a symptom screen, chest X-ray or molecular WHO recommended rapid diagnostic tests, alone or in combination. The advent of ultra-portable digital X-ray machines and computer aided technology will quickly lead to the actualisation of these guidelines. How will the implementation be done? What other conditions will the use of CXR identify? How should health systems be prepared for these conditions? These are among the questions that arise as countries plan for the implementation of CXR for TB screening.
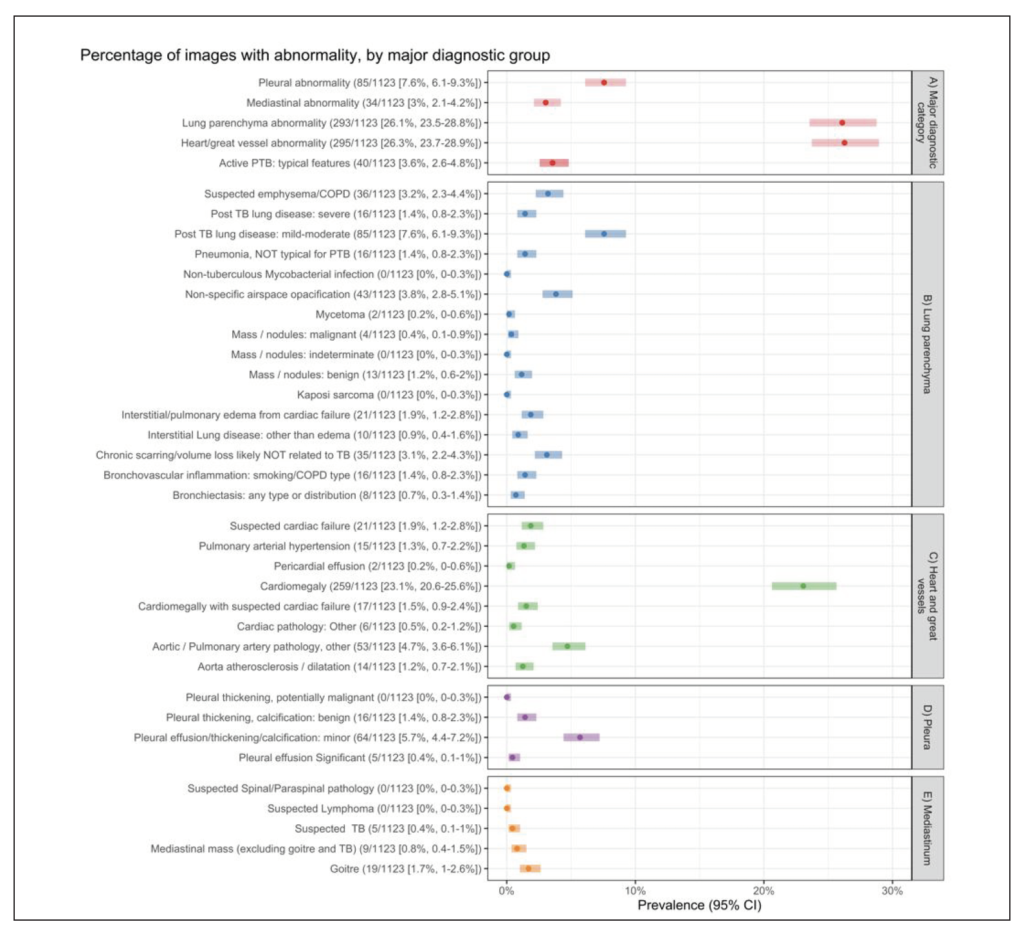
In 2019, we conducted a study to describe and quantify non-TB abnormalities identified by TB focused CXR screening during the 2016 Kenya National TB Prevalence Survey. We reviewed a random sample of 1140 adult (≥15 years) CXRs classified as “abnormal, suggestive of TB” or “abnormal other” during field interpretation from the TB Prevalence Survey. Each image was read by two expert radiologists, with images classified into one of four major anatomical categories and primary radiological findings. A third reader resolved discrepancies.
From our findings, we identified other conditions, especially those related to complications of a rising burden of non-communicable diseases (NCDs). These included cardiomegaly (enlarged heart), suspected chronic obstructive pulmonary disease, post-TB lung changes and other nonspecific lung patterns.
Implications of Our Findings
In sub-Saharan Africa, the commonest causes of cardiomegaly are conditions of significant public health importance associated with premature mortality, including: hypertensive heart disease; cardiomyopathies; cor pulmonale; chronic rheumatic heart diseases; and ischaemic heart diseases. (2, 3) Cardiomegaly has been associated with both higher body mass index (BMI) and higher median systolic blood pressure (BP).(4) The high prevalence of cardiomegaly in our study supports exploration of the benefits of CVD screening during TB CXR screening as a potentially affordable public health intervention.(3, 5) Health messaging on prevention of NCDs through recommendations on diet, such as reduction of commercial sugar and high salt diet, could be considered for integration in such programmes.(3)
We recommend that clear referral pathways, diagnostics and followup plans for non-TB pathology be incorporated during the planning of TB active case finding activities.
Prospective data collection about non-TB condition identified during TB screening, characterisation of these patients, exploration of individual and health systems implications of these diseases could assist with further planning. Our findings were consistent with complications of potential underlying NCDs, including chronic respiratory disease in the population. At primary care health facilities, prevention efforts for NCDs should be strengthened including health messaging, BP and BMI monitoring.
In conclusion, mass radiography can be used to tackle “fundamental problems of disease in the chest, both of the respiratory system and also of the heart” and “aid in detection of early and treatable non-TB disease”.(5) As countries embark on TB ACF activities, they need to be aware that other respiratory and non-respiratory pathologies are likely to be as, or more prevalent, than active TB. Mass screening with CXR therefore offers opportunity to plan for and address multiple important diseases.
- WHO. WHO consolidated guidelines on tuberculosis. Module 2: screening – systematic screening for tuberculosis disease. Geneva:World Health Organization 2021.
- Akosa AB, Armah H. Cardiomegaly in Ghana: An Autopsy Study. Ghana Med J. 2005;39(4):122-7.
- Mensah GA, Roth GA, Sampson UK, Moran AE, Feigin VL, Forouzanfar MH, et al. Mortality from cardiovascular diseases in sub-Saharan Africa, 1990-2013: a systematic analysis of data from the Global Burden of Disease Study 2013. Cardiovasc J Afr. 2015;26(2 Suppl 1):S6-10.
- Esmail H, Oni T, Thienemann F, Omar-Davies N, Wilkinson RJ, Ntsekhe M. Cardio-Thoracic Ratio Is Stable, Reproducible and Has Potential as a Screening Tool for HIV-1 Related Cardiac Disorders in Resource Poor Settings. PloS one. 2016;11(10):e0163490-e.
- Maxwell J, Kerley P, Paxon T. Discussion on non-tuberculous conditions revealed by mass radiography. Proc R Soc Med.1949;42(12):1039-44.
- Mungai BN, Joekes E, Masini E, Obasi A, Manduku V, Mugi B, et al. ‘If not TB, what could it be?’ Chest X-ray findings from the 2016 Kenya Tuberculosis Prevalence Survey. Thorax. 2021.
The findings from our study were published in 2021 https://pubmed.ncbi.nlm.nih.gov/33504563/ (Mungai BN, Joekes E, Masini E, et al. ‘If not TB, what could it be?’ Chest X-ray findings from the 2016 Kenya Tuberculosis Prevalence Survey. Thorax. 2021).(3) This research was funded by the National Institute for Health Research (NIHR) (IMPALA), grant reference 16/136/35) using UK aid from the UK Government to support global health research. The views expressed in this publication are those of the author(s) and not necessarily those of the NIHR or the UK Department of Health and Social Care.
{kind=link}
{kind=link}